
In 2008, researchers from Peking University Medical Science History Research Center introduced the historical story of China [barefoot doctors] to the world for the first time in the form of formal papers.
This commentary, published in the famous medical journal Lancet, is entitled:
China’s barefoot doctor: pass, present, and future
The article collected the data of rural medical personnel and institutions in China from 1950 to 2000, and drew a picture of the past and [present].
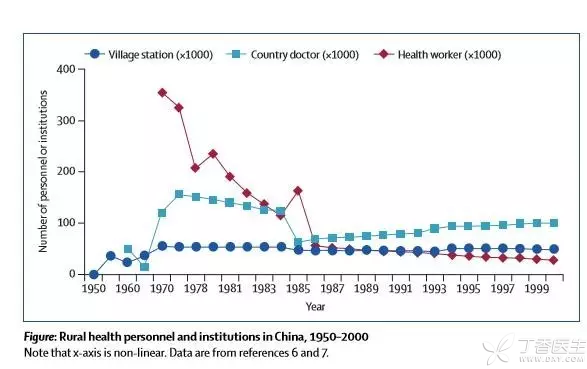
The “Barefoot Doctors” program to improve rural medical conditions was launched in 1965 and abolished in 1985. Some of these barefoot doctors left the medical industry while the rest became rural doctors.
More than ten years have passed since the publication of the paper, and [barefoot doctors] have become historical terms. But is there any concern about the situation of [rural doctors] in China?
The hardest doctor
Although the working environment in most hospitals is not ideal, at least, there is no need to get cold in winter and not too hot in summer. Doctors working indoors can hardly understand the feeling of carrying medicine boxes over mountains, sliding over iron rope bridges and practicing medicine in heavy rain or snow.
This is the epitome and true portrayal of the practice of more than one million rural doctors across the country.
A village doctor is often responsible for the medical tasks of the people in several villages, with a wide range and a long journey.
Those with better conditions can ride electric vehicles, motorcycles and bicycles. The more remote villages and the more remote mountainous areas can only be walked. The mountain roads and waterways that come and go for dozens of miles can really be described as wading across mountains and rivers, and the difficulties can be imagined.
However, the difficulties of rural doctors are not only the difficulties in the natural environment:
1. Unidentified:
Doctor or farmer? This is what puzzles many village doctors.
In many areas, in addition to practicing medicine, rural doctors have to rely on farming to support their families and improve their lives. There are also some rural doctors who work as doctors and bear the risks of doctors, but what they enjoy is the low treatment of farmers.
2. Heavy task:
Rural doctors not only have to take on the medical work of neighbors, but also need rural doctors to be responsible for public health tasks, such as vaccination, infectious disease prevention, physical examination, health education, file management, etc.
Rural doctors are often tired of the small number of personnel and heavy workload.
Rural doctors have no holidays or weekends. No matter late at night or early in the morning, as long as there are patients seeking medical treatment or calling for medical treatment, they have to go out immediately and be on call. Rest and sleep are not guaranteed at all.
3. Low treatment:
In many areas, the salaries of rural doctors are very low, only about 1,000 yuan, and in some places even only a few hundred yuan, still struggling on the poverty line.
In desperation, village doctors had to rely on farming or other businesses to support their families and make a difficult living.
In the end, the village doctors did not take over and there was no successor. Only the elderly and infirm village doctors were left. They were unable to change their careers and were unable to change their minds at first sight. They devoted the rest of their lives with difficulty.
4. The risks are enormous:
Medical treatment itself has great risks and uncertainties.
In developed hospitals, with experienced doctors and advanced medical equipment as backing, risks are relatively easy to control. However, rural doctors, who are short of rescue equipment and professional skills, can only feel powerless when faced with various variables that may exist in medical treatment.

Retaining rural doctors cannot rely solely on feelings.
[Most Beautiful Country Doctor] Mary once told such a story:
Because of the difficult conditions, and because I tumbled down the cliff on my way back to the health station after a visit, I lost my child who was only three months pregnant, which was even more serious. Sadly, because of this, I also lost the right to be a mother forever.
At this time, I had the idea of leaving. On the morning of leaving, as soon as I opened the door, the door was already full of villagers who had come to see me off overnight. They came from ten miles and eight villages to see me off. Looking at familiar faces and helpless eyes, I was somewhat at a loss.
Suddenly, a tearful child ran out of the crowd, hugged my thigh tightly and cried, “Mammy Ma, don’t go, don’t go!” I don’t want you to go …] This is the first child I delivered with my own hands. Now I am almost 5 years old.
Seeing this, we said that what finally retained Mary, a village doctor, should be said to be feelings, feelings, and the trust, love, even dependence and attachment of simple villagers and children to Mary.
Doctors stayed and continued to sacrifice slowly in difficult positions. It is touching to keep people with emotion, but it is not a long-term plan to keep rural doctors.
Rural doctors need better treatment.
The management system of rural doctors in line with the characteristics of the times needs to have a reasonable orientation for rural doctors in terms of labor relations, old-age insurance, practice risks, wages and other aspects, so as to effectively improve the social status and economic treatment of rural doctors and create a good practice environment for them.
The design of these systems requires top-level and top-level managers to follow the objective reality and come to the conclusion through the actual investigation of the grassroots, instead of fabricating them out of thin air and working behind closed doors.
However, at present, the decrease in the income of rural doctors is precisely partly caused by policy reasons. For example, in 2009, the state implemented the basic drug system and abolished the drug addition. This is undoubtedly a [big benefit] for the vast number of patients. However, for village doctors who rely on selling drugs to obtain the difference as their main source of income, it has become a factor leading to a sharp drop in income.
Attracting talents to stay with better treatment is the most reliable means in this era. However, with treatment, medical talents are also needed.
Medical education should last for a lifetime.
There is also an important reason why rural doctors are short of successors: lack of opportunities to receive continuing education and lifelong education, lack of improvement in professional knowledge, and slim prospects for development.
Even if a village doctor and a doctor from a 3A hospital graduate from the same school and degree, five years later, the mastery of their professional knowledge and skills can be said to be quite different.
What’s more, rural doctors and doctors in 3A hospitals do not have the same starting point at all.
In 2015, BMC Medical Education included 1,197 rural doctors from Liaoning in its last paper on lifelong learning of rural doctors in China, but only 3.5% had bachelor’s degree or above. Liaoning is not a backward area in the traditional sense.
Therefore, the continuing education of rural doctors is especially important. Experts go down and sink to the grassroots to pass, help and take care of them. Village doctors go up and receive free training in higher-level hospitals.
Only in this way can rural doctors be truly strengthened.